Surgi-ORC® in Chronic Subdural Hematoma: Advancing Surgical Outcomes
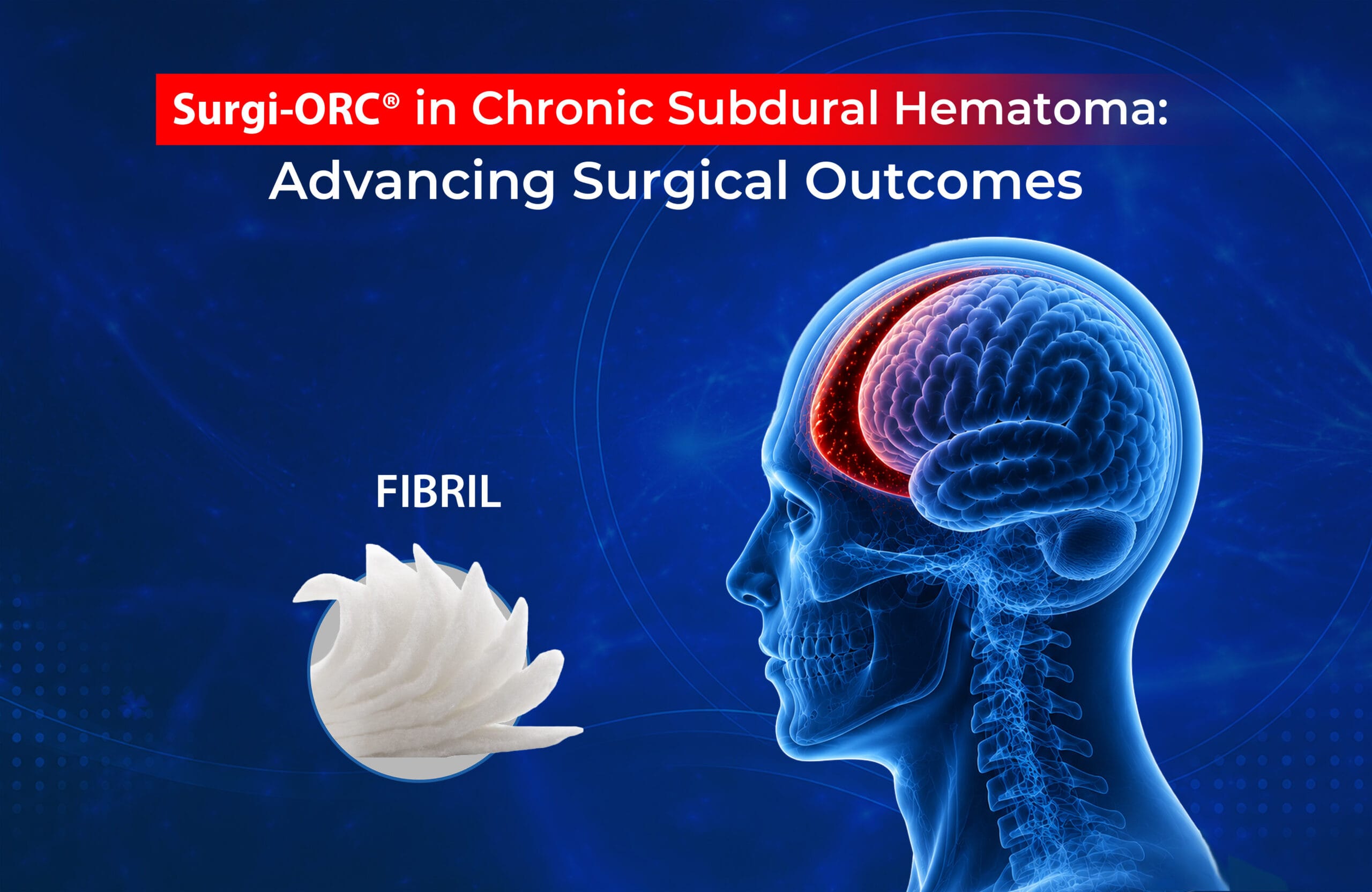
A chronic subdural hematoma (cSDH) is a slow collection of blood and blood degradation products between the layers covering the brain.1,2 It often happens after a minor head injury, typically represents in adults. Over time, the pressure from this blood can affect the brain, leading to symptoms like headaches, confusion, or weakness. The image below shows where this type of bleeding can occur.1
Figure 1: Different Forms of Subdural Hematoma1
What Makes cSDH Surgery Challenging?
cSDH is primarily treated with surgical evacuation using techniques such as burr holes, craniostomy, or mini craniotomy with or without membranotomy and standard hemicraniectomy. However, symptomatic recurrence remains a major challenge. Persistent micro bleeding drives this issue, leading to the following concerns:2-5
- Recurrence due to fragile neomembrane bleeding
- Higher risk in multilayered cSDH (laminar, separated, gradation types)
- Patients often trapped in a cycle of repeated surgery
- Patient-related factors such as tissue fragility, high surgical risk, and anticoagulant use, increasing bleeding complications
This highlights the need for an adjunctive solution that not only controls bleeding but also supports long-term stability. In such cases, products like oxidized regenerated cellulose (Surgi-ORC®) can play a role in managing multilayered cSDH. Therefore, Let’s explore Surgi-ORC® and how this technique is applied in treatment.
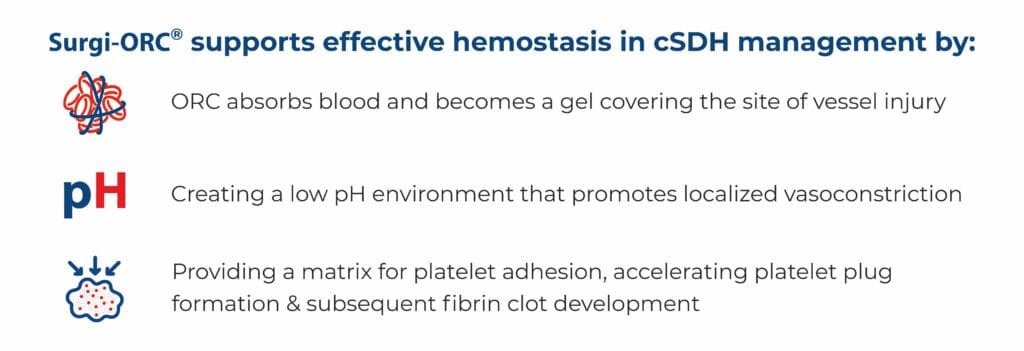
How Does Surgi-ORC® Work?
Surgi-ORC® is a natural, plant based absorbable haemostat made up of oxidized regenerated cellulose, designed to stop capillary, venous and minor arterial bleeding. The fibrillar form is used during such surgery to enhance surface contact and promote effective haemostasis.

Figure 2: Surgi-ORC® FIBRIL- Absorbable Haemostat (Oxidized Regenerated Cellulose)
 ORC Supporting Surgical Precision:
ORC Supporting Surgical Precision:
Incorporating ORC into advanced techniques, such as membrane tucking with intermembranous placement, provides a targeted approach to address the source of bleeding. This method helps stabilize the subdural space and may reduce the likelihood of recurrence.2
What Does a Clinical Experience Show?
Emerging evidence supports the use of ORC as an adjunct in cSDH surgery. In a study of 23 patients with multilayered cSDH confirmed on preoperative MRI, the novel surgical technique was applied. The cohort had a mean age of 61.34 years, a male-to-female ratio of 4.75:1, and included laminar (26.08%), separated (56.52%), and gradation (17.39%) type cSDH. Stepwise surgical technique for multilayered cSDH:2

Figure 3: (a) After craniotomy and durotomy, the dura is dissected from the external membrane (b) Membranes are carefully incised and separated. (c) Margins are trimmed, and the intermembranous space is exposed and irrigated.2
 Figure 4: (a) ORC Fibrillar is placed between layers. (b) All membranes are tucked together with intermembranous ORC and secured to the dura using Ligaclips. (c) The dura is closed (non–water-tight) and the bone flap is placed back over the craniotomy defect.2
Figure 4: (a) ORC Fibrillar is placed between layers. (b) All membranes are tucked together with intermembranous ORC and secured to the dura using Ligaclips. (c) The dura is closed (non–water-tight) and the bone flap is placed back over the craniotomy defect.2
Key observations:2
• 0% postoperative recurrence, assessed at day 1 and 3-month follow-up scans
• 0% reoperation rate in this series
• 0% ORC-related complications, with no adverse events from ORC or Ligaclips
The technique combining membrane tucking with ORC Fibrillar placement was found to be safe, effective, and reproducible, with potential to reduce recurrence.²
Conclusion
Surgi-ORC® offers a simple and practical addition to cSDH surgical management. By helping control ongoing microbleeding, it supports better stability and may reduce the risk of recurrence. As an adjunct to standard and novel techniques, it contributes to more consistent, reliable, and improved patient outcomes. Its ease of use and adaptability make it a valuable option in routine neurosurgical practice.
References:
1. Chronic subdural haematoma (cSDH) | CUH
2. Singh L, Agrawal N, Multani KM. Membrane tucking technique using ligature clips with intermembranous placement of oxidized regenerated cellulose (SURGICEL®, FIBRILLAR) in multilayered chronic subdural hematoma: Description of novel technique and our initial experience. Neurology India. 2023 Mar 1;71(2):267-71. DOI: 10.4103/0028-3886.375434
3. Perini Durigan, Á., de Paula Simoni, M., Braga, N., Garg, K., Chavez-Herrera, V. R., Eduarda Pommer, M., de Paula Simoni, L., Henrique Simoni, G., Susin, G., & Chaurasia, B. (2025). Evolution of surgery for chronic subdural hematoma: a narrative review. Annals of medicine and surgery (2012), 87(7), 4139–4144. https://doi.org/10.1097/MS9.0000000000003324
4. Nakaguchi H, Tanishima T, Yoshimasu N. Factors in the natural history of chronic subdural hematomas that influence their postoperative recurrence. J Neurosurg 2001;95:256‑62. DOI link: https://doi.org/10.3171/jns.2001.95.2.0256
5. Tiwari DP, Sharma V, Raj J. Multiple density subdural hematomas. Open J Modern Neurosurg 2014;4:4. doi: 10.4236/ojmn.2014.41004. DOI: 10.4236/ojmn.2014.41004