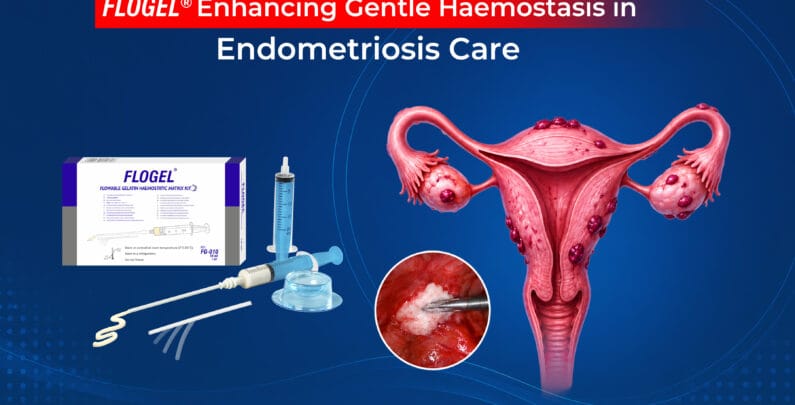
FLOGEL® Enhancing Gentle Haemostasis in Endometriosis Care
Endometriosis is a common, benign, estrogen-dependent condition affecting women of reproductive age. It often presents as ovarian endometriomas and may be associated with pelvic pain, dysmenorrhea, dyspareunia, infertility, or may be discovered incidentally during imaging or surgery.1,2
Surgical treatment options include fenestration with coagulation, laser vaporization, and laparoscopic cystectomy. Among these, cystectomy is generally considered the preferred approach, as it has been shown to reduce recurrence compared with drainage and ablation and is associated with better fertility outcomes.2,3 However, once the cyst is removed, achieving effective haemostasis from the ovarian bed can still be a challenging step in the procedure.
Why does the choice of haemostatic method matter in endometrioma surgery?
The method used to control bleeding during laparoscopic cystectomy for endometriosis can directly affect ovarian tissue. Choosing an approach that ensures effective haemostasis while minimizing tissue damage is essential to preserving ovarian function and long-term outcomes. After stripping the cyst wall, the subsequent bleeding of the ovarian stromal wound is usually controlled by bipolar coagulation or/and by suturing.4 The table below outlines the impact of different haemostatic methods on ovarian tissue.2-5
Table 1: Haemostatic Methods and Their Impact on Ovarian Tissue
| Method | Mechanism | Impact on Ovarian Tissue and limits |
| Bipolar coagulation | Thermal energy for vessel sealing | May negatively affect ovarian reserve, particularly in large ovarian beds, due to the risk of thermal follicular damage.3,5 |
| Ultrasound scalpel coagulation | High-frequency ultrasonic energy causing protein denaturation and tissue cutting/coagulation | Similar concerns regarding ovarian reserve preservation as bipolar coagulation, along with higher equipment costs.5 |
| Laparoscopic suturing | Mechanical approximation and compression of tissue for haemostasis | Technically challenging, requiring added dexterity and training, and may prolong operative time, and can increase tissue injury with higher intra-ovarian pressure and ischemic risk.4,5 |
| Haemostatic matrix / Sealant | Topical mechanical haemostasis | Preserves ovarian function better than bipolar electric coagulation or electrocautery.3,5 |
To make this step more tissue-friendly, surgeons are increasingly using topical haemostatic agents such as gelatin-based matrices (e.g., FLOGEL®). These agents help achieve effective bleeding control by promoting natural clot formation while minimizing trauma to the surrounding ovarian tissue, making them a useful support in ovarian endometrioma surgery.
What is FLOGEL®?
FLOGEL® is a flowable gelatin-based haemostatic matrix supplied in a prefilled syringe for fast bleeding control, usually within 2–5 minutes. The flowable nature of FLOGEL allows it to conform to irregular wound surfaces and reach difficult-to-access areas.

Figure 1: FLOGEL® Flowable Gelatin Haemostatic Matrix Kit
It closely adapts to the bleeding site and can be combined with thrombin to enhance and accelerate the body’s natural clotting process. By providing effective haemostasis without thermal injury, it offers a practical and tissue-friendly alternative to electrosurgical methods.
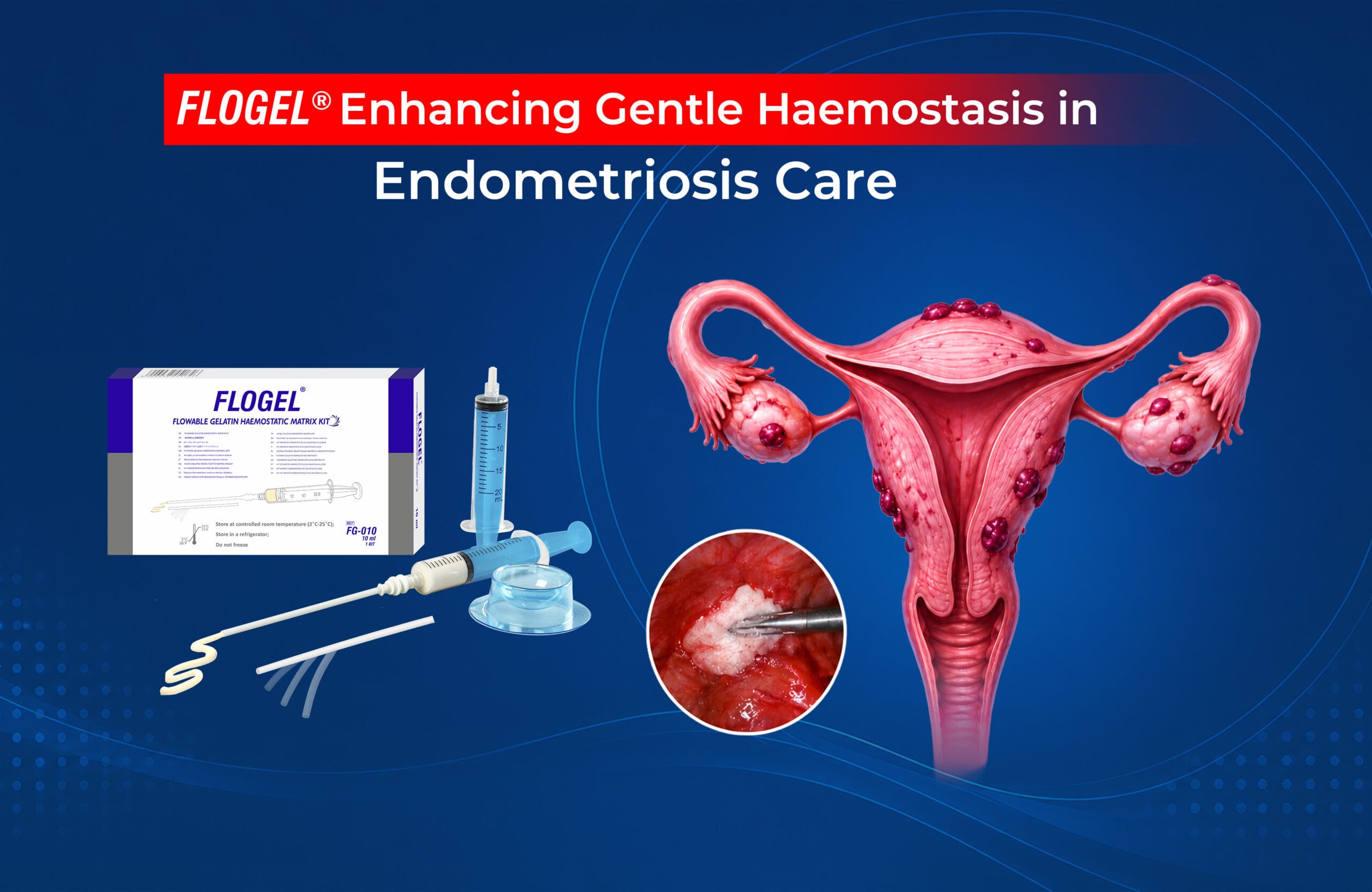
What are the key features?
What does clinical evidence suggest?
A study of 20 patients undergoing laparoscopic endometrioma excision (cyst diameter 3–6 cm) compared haemostasis using a gelatin–thrombin matrix (n=8) with conventional haemostatic methods (bipolar forceps or CO₂ laser, n=12).
Key findings:3
Haemostasis was achieved in all cases within 3 minutes, with comparable outcomes to conventional methods (172 vs 182 seconds (about 6 minutes)) and no intra- or postoperative complications, bleeding, or transfusion requirements were reported.3
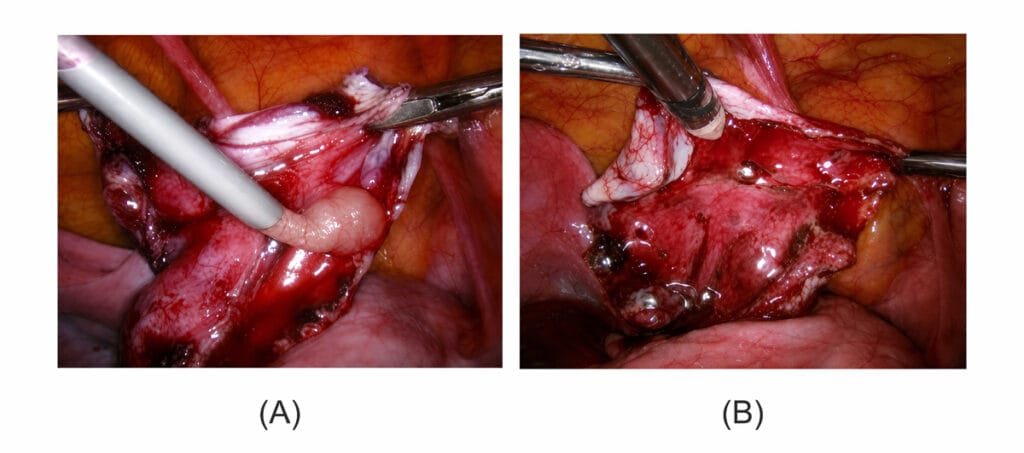
Figure 2: (A) Sites of bleeding covered with gelatin–thrombin matrix (B) Anpexal wall after gelatin–thrombin matrix application.
The study suggests that topical gelatin–thrombin matrix haemostatic agents may be a useful alternative to bipolar coagulation to reduce thermal damage to follicular or ovarian tissue and may help better preserve ovarian reserve after laparoscopic cystectomy for endometriosis.2,3
Conclusion:
FLOGEL® provides effective haemostasis during endometriosis surgery while avoiding thermal injury associated with bipolar coagulation. By supporting natural clot formation and minimizing damage to ovarian tissue, it may help preserve ovarian reserves following cystectomy. Its flowable, tissue-friendly design makes it a valuable adjunct for achieving gentle and effective haemostasis in ovarian endometrioma surgery.
References:
- Endometriosis – Symptoms and causes – Mayo Clinic
- Choi C, Kim WY, Lee DH, Lee SH. Usefulness of hemostatic sealants for minimizing ovarian damage during laparoscopic cystectomy for endometriosis. Journal of Obstetrics and Gynaecology Research. 2018 Mar;44(3):532-9. doi:10.1111/jog.13542
- Angioli R, Muzii L, Montera R, Damiani P, Bellati F, Plotti F, Zullo MA, Oronzi I, Terranova C, Panici PB. Feasibility of the use of novel matrix hemostatic sealant (FloSeal) to achieve hemostasis during laparoscopic excision of endometrioma. Journal of minimally invasive gynecology. 2009 Mar 1;16(2):153-6. doi:10.1016/j.jmig.2008.11.007
- Ebert AD, Hollauer A, Fuhr N, Langolf O, Papadopoulos T. Laparoscopic ovarian cystectomy without bipolar coagulation or sutures using a gelantine-thrombin matrix sealant (FloSeal): First support of a promising technique. Arch Gyne col Obstet 2009; 280: 161–165. DOI 10.1007/s00404-009-0985-4
- Grammatis AL, Lazaridis A, Becker CM, Saridogan E. Surgical techniques for ovarian endometriosis. The Obstetrician & Gynaecologist. 2024 Sep 26. DOI: 10.1111/tog.12947